[Based on research and excerpts from “Save Dogs From Distemper: The ‘Impossible’ Cure of Dr. Alson Sears”]
By Ed Bond
The battle to save dogs from canine distemper has been complicated by historic problems in identification and diagnosis, recognizing the cause, developing an effective vaccine, finding effective treatments and understanding how and when a dog with distemper can survive. By unraveling these problems, we may see the value in studying emerging treatments with a goal of significantly increasing survival rates.
History of the virus
Edward Jenner, the English physician who documented the first cowpox vaccination against small pox, made remarkable progress on the first problem of identification and diagnosis in 1809 when he wrote the first scientific paper on canine distemper and established it as a disease separate from rabies. When the hounds of the Earl of Berkeley fell ill, he studied them carefully because of an incident in his youth.
He wrote:
“It may be difficult, perhaps, precisely to ascertain the period of its first appearance in Britain. In this and the neighbouring counties, I have not been able to trace it back much beyond the middle of the last century; but it has since spread universally. I knew a gentleman who, about forty-five years ago, destroyed the greater part of his hounds, from supposing them mad, when the distemper first broke out among them; so little was it then known by those the most conversant with dogs.” (Jenner 1809)
While scientists and veterinarians had confused various outbreaks of dog disease throughout history as the possible origin of distemper, it turns out Jenner had not been too far off in his description. Modern researchers have determined the disease did begin in the 18th century, but in South America, not in Europe.
A paper published in the International Journal of Paleopathology in March 2019 used modern methods to determine canine distemper evolved as a mutation of the measles virus in South America during the period of European colonization.[1] The Spanish explorers brought diseases like measles and small pox to the New World, and these viruses became unwitting allies in the conquest of the Americas.
The modern researchers point to an outbreak of canine distemper around Quito in 1746. Native populations of dogs almost disappeared during the period of European colonization in an epidemic similar to that ones that devastated the native human population.
The new virus made its way to Europe. In 1760, 900 dog deaths were reported in Madrid on a single day. By the mid-1760s, the disease had reached Great Britain where a young Edward Jenner, then a teenager and apprentice surgeon, would witness one of the first outbreaks.
The horror of rabies – also known as hydrophobia – had been known since ancient times. The name hydrophobia comes from the overpowering fear of water victims of rabies suffer from. This is one of the devastating symptoms of the disease, which also caused convulsions, hallucinations and fits before death.
In the 18th Century, wiping out a pack of dogs to stop the spread of rabies made sense, not only to save other dogs but also to save humans from a horrible fate. But an assumption of rabies was not enough to satisfy Jenner.
From his observations of the hounds of the Earl of Berkeley, he described the disease as beginning with an inflammation of the lungs, vomiting and diarrhea. A dark mucous covered the teeth. The eyes were inflamed and also covered with mucous. In his paper, “Distemper in Dogs,” he goes on to write:
“The brain is often affected as early as the second day after the attack. The animal becomes stupid, and his general habits are changed. In this state, if not prevented by loss of strength, he sometimes wanders from home. He is frequently endeavoring to expel, by forcible expirations, the mucus from the trachea and fauces, with a peculiar rattling noise. His jaws are generally smeared with it, and it sometimes flows out in a frothy state, from his frequent champing. During the progress of the disease, especially in its advanced stages, he is disposed to bite and gnaw any thing within his reach. He has sometimes epileptic fits, or quick succession of general, though slight convulsive spasms of the muscles. If the dog survives, this affection of the muscles continues through life. He is often attacked with fits of a different description. He first staggers, then tumbles, rolls, cries as if whipped, and tears up the ground with his teeth and forefeet.” (Jenner 1809)
To any other English gentleman of this time, these symptoms might be enough to justify a conclusion of rabies. But Jenner continued to study these animals. He noted:
· The dogs were not afraid of water. He said of one: “his thirst seems insatiable, and nothing seems to cheer him like the sight of water.”
· This disease was not communicable to humans.
As to the survivability, distemper “cuts off, at least, one in three that is attacked by it,” he wrote.
Its very name had been born out of ignorance and superstition and apparently predates the emergence of the actual disease by a few centuries.
The English word distemper came from the Old French word destemprer (late 14th century) meaning “to disturb” and the earlier Medieval Latin word distemperare “vex, make ill.” In the Middle Ages, any illness was thought to be caused by a disturbance of the four bodily humors – Yellow Bile, Black Bile, Phlegm and Blood. So, distemper – disturbance of the humors – began as a catchall term for any illness in a human or animal. As other diseases were identified and named, distemper ended up with its name by default.
Figuring out the cause of canine distemper would take another century. Again, it would take a lot of guesswork and overcoming the wrong assumptions.
The first scientists searching for the cause of canine distemper encountered plenty of bacteria. Beginning in 1875, researchers reported finding various microscopic candidates they thought were responsible for canine distemper. Between 1875 and 1910, nearly two-dozen theories had been proposed. Most of these were bacteria.[2]
Among the din of claims was a report by a 35-year-old French scientist named Henri Carré, director of the Research Laboratory of Maisons-Alfort outside of Paris. Through experimentation, he concluded in 1905:
· Distemper was a filterable virus.
· It could be found in the watery nasal discharge (and some other fluids) of the sick dog.
· Two or three drops were enough to induce the disease and often death.
· There was no organism that could be cultivated.
· Survivors would be immune to further attacks.
However, the idea of a virus was still new. Bacteria were relatively easy to recognize because they could also be grown in cultures outside of a host body. 19th Century scientists would pass infectious material through a porcelain filter, and if the resulting material were no longer infectious, they’d know the bacteria had been stopped by the filter and were therefore bigger than its holes.
But then researchers discovered sap from a diseased tobacco plant could pass through any bacterial filter and still be infectious to healthy tobacco plants. In 1898, this unseen agent became the first recognized plant virus. [3]
Viruses were a difficult concept for 19th Century scientists because they could not be seen under a microscope and they could not be grown in culture. Compared with a bacterium, a virus is miniscule. Bacteria are complete cells. Viruses are merely small packets of genetic material that invade living cells to replicate themselves. They would not be seen directly until the first electron microscopes in the 1930s.
So Carré could not actually show the world his distemper virus. And for years after he made his claim, most veterinarians assumed distemper was some form of bacteria. In 1910, American researcher Newell S. Ferry and British researcher J.P. M’Gowan reported that the agent responsible was Bacillus bronchisepticus, which was at the time one of the smallest known organisms. (Ferry 1911; M’Gowan 1911) Work by other researchers supported this conclusion. For someone in the 21st Century, the reason for the confusion is obvious. The distemper virus knocks down the immune system and this allows bacterial diseases to attack. These early researchers were finding the bacteria taking advantage of the distemper attack, not the attack itself. In fact, Bacillus bronchisepticus is a known cause of pneumonia, which shows up in distemper dogs.
Throughout this period, researchers made several attempts to either prevent the spread of the disease or to find a cure. These included:
· Cow-pox vaccination, which failed.
· Inoculating the healthy dog with the nasal discharge of a sick dog – or having the dogs make nose-to-nose contact – as a form of variolation. This usually killed the dog they were trying to protect.
· Copeman’s Vaccine, which in 1900 was derived from a broth culture of bacteria from a distemper dog. Dr. Monckton Copeman’s product was sometimes called an “anti-distemper serum.”[4]
In 1922, the veterinary and scientific communities were still grasping at straws over the problem of canine distemper when British veterinarian Hamilton Kirk wrote a book summarizing what was then known about the disease. At the time, the cause was still very much in debate. He wrote:
“In the discovery of a prophylactic or curative vaccine or serum lies the only hope of salvation for the canine race against the dread scourge of distemper, and the bacteriologist who can accomplish this will deservedly become famous in the annals of veterinary science.” [5]
Despite his expressed hope for either a preventative or a cure, Kirk had strong words for “quack remedies.”:
“In view of the diversity of this disease, it must be obvious to all how impossible it is to expect to derive benefit from any one prescription. Each case must be treated on its merits, and since no specific therapeutic agent exists, one must necessarily treat the symptoms as they arise.” [6]
Kirk then goes on in detail to describe the supportive nursing care for distemper dogs, including the need for hygienic conditions, keeping the animal warm, using steam kettles, proper diet and medications to treat symptoms as they occur.
“Saving the lives of our dogs”
In 1923, The Field, a weekly country journal for sportsmen, landowners and farmers in Britain published an appeal for a distemper fund to support a massive research project to save dogs from canine distemper. This appeal was made out of a love of dogs as much as for a need to advance medical science. Members of the landed aristocracy and others donated £55,000 – £8.8 million in today’s economy – which was spent on distemper research between 1923 and 1932. [7]
The research happened through a collaboration between veterinary professionals, the Medical Research Council and Burroughs-Wellcome, a pharmaceutical company. At the center of the effort were two pathologists named Patrick Laidlaw and G.W. Dunkin. Their first job was to settle the argument about the cause of canine distemper. Dogs were bred specifically to be free of diseases on a farm at Mill Hill in North London to ensure no other pathogen was affecting the results.
Through experiments in which healthy puppies were exposed to dogs infected with distemper, they were able to rule out Bacillus bronchisepticus as the cause of canine distemper. By early 1926, they concluded ‘the infecting agent of dog-distemper belongs to the class of filter-passing viruses.’
So after more than 20 years, Carré’s theory had been validated, and later academic papers would refer to distemper as the “Virus of Carré” until viruses were reclassified in the latter part of the 20th Century.[8]
But Laidlaw and Dunkin now had to develop an effective vaccine, and they decided dogs were not suitable as long-term laboratory animals. They did not endure the isolation well.
Ferrets, another canid susceptible to distemper, proved to be more useful because they thrived in small spaces and bred quickly. In their research, they found the spleen of the ferret collected the most virus and was the most useful to create a vaccine for other ferrets.
The ferret vaccine did not translate well over to dogs. So, they created a dog version by grinding up the spleen, liver and glands of infected distemper dogs. This created a viral extract that would then be treated with formalin. The inactive virus would then become the vaccine that would trigger the immune system of healthy dogs to recognize the distemper virus and stop them from getting the disease.
They found the best way to vaccinate would be to first use the inactive version of the virus, followed two weeks later with the full-strength version. Early trials in estates, homes and kennels were encouraging. Distemper cases were cut to 1 out of 100 vaccinated dogs. But problems arose in ensuring the consistency of how the double dose of vaccine was used, and the first commercial version of the vaccine was pulled from the market after only 16 months.
But this was enough for The Field to declare victory. On Feb. 4, 1933, The Field published a twelve-page special supplement celebrating the conquest of canine distemper: ‘Saving the lives of our dogs.’ However, the first reliable commercial version of the vaccine would not be developed until 1950.
The scientific search to save dogs from distemper apparently ended with the development of the canine distemper vaccine. Dogs could be saved from the disease if vaccinated in time. But if already sickened, vets had to rely on supportive methods, treat each symptom as it arose and hope for the best. Dogs that reached the neurologic stage of the disease were euthanized. A cure for distemper became seen as unnecessary, impossible and likely quackery.
But unlike the small pox vaccine, the development of a canine distemper vaccine would not end the virus. When the World Health Organization launched its final assault on small pox in 1967, they had a key strategic advantage: Small pox only infected humans. Teams of vaccinators could travel the world and vaccinate every human in areas at risk. They could track the disease, and in 1977 when the last scab fell off the last victim of the disease – a Somali hospital worker – they knew they were close to finishing off their foe. WHO declared complete victory over small pox in 1980.
Distemper does not sicken humans, but it can infect a wide range of canid animals (dog, fox, coyote, wolf) as well as large wild cats, river otters, bears and even Rhesus monkeys. The distemper virus exists wherever there are carnivores. Domestic dogs – the most numerous of carnivores on the planet at more than 500 million – are the main reservoir for canine distemper. This means they are the animal population where the virus is naturally found, from where it grows and spreads to other susceptible species. Raccoons are considered to be a secondary reservoir for the disease.
So, even with perfect vigilance and nearly complete vaccination of domestic dogs, the virus would most likely still be waiting to attack from the surrounding wildlife. Treatment options are still needed.
A potential treatment
In 1972, Dr. Alson Sears, a veterinarian in the desert community of Lancaster, California, read the research on using Newcastle’s Disease Vaccine (NDV) as an inducer to boost levels of interferon in cats. The major dog disease he faced in his storefront clinic was distemper. Dr. Sears had followed the officially sanctioned treatments for distemper – fluids, antibiotics, and watching them die.
“Most of the dogs that came in with distemper died,” he said. “We’re talking many, many, many boxes of dead dogs. Those that did survive went on to see horrible secondary neurologic problems from which many lingered and eventually died. Once sick, there did not seem to be much that could be done to help them.”
When he read about the NDV research in cats, “It clicked in my head that this might work against distemper. I thought, ‘Damn, if it works in cats, here’s a viral technique we haven’t tried.’”
Dr. Sears borrowed a healthy dog from the local shelter, and he bought a box of NDV vaccine at an agricultural store.
After injecting about 2 to 3mls of NDV into the vein of the donor dog, Dr. Sears waited until the next day to collect serum. The dog was anesthetized and placed on a splint designed to hold it on its back on a surgical table. An IV was set up to keep fluids going into the dog’s body. The dog’s neck was shaved and a catheter inserted into the jugular vein to withdraw blood into vials. A centrifuge was used to separate the blood serum from the blood cells.
“But there was a hitch, which at the time we didn’t recognize,” he said. “Time.”
He had done all of this without realizing the journal article on interferon he was trying to follow had called for the serum to be withdrawn 6 to 8 hours after the injection. Dr. Al Sears had waited 11½ to 12 hours.
“I pulled it off at the time I thought was appropriate,” Al says. “What did I know? We’d never done this before.”
Looking back, he calls the change in timing serendipity. Perhaps, it was a happy accident of science. “Some mistakes are beneficial and some mistakes are not,” Dr. Sears said. “In this case, the mistake was hugely beneficial.”
They returned the blood-serum donor dog to the shelter, unharmed, and stored the vials of serum in the clinic’s refrigerator. He sent a sample to Cornell University and asked them to check whether it contained interferon. Four days later, a client brought in a canine distemper case, a 6- to 8-month-old shepherd-lab mix that had never been vaccinated.
“He came in with a real nice acute case,” he said. “One of the classics, you know. You get a high fever. He had a little diarrhea and vomiting and a runny nose, gooped up eyes, and a cracked nose. He was just a classic.”
Without time to get the response from Cornell, Dr. Sears didn’t know whether the serum in his refrigerator had interferon. But he had a patient likely to die without treatment, and he needed to know whether this material worked.
Late that afternoon, he injected the serum into his patient subcutaneously. The patient was returned to its cage for the night. “I figured, ‘We’ll see,’ ” he said.
In the morning, the dog bounced around happily. “The dog was jumping up and down in the cage, and its nose was cleared up, and its eyes were cleared up,” he said. “His fever was gone. I put him down on the floor and he ran around. We put some food out and he jumped into the food like he hadn’t eaten for three or five days, which he probably hadn’t. I’m looking at the dog and thinking, ‘Geez, this dog’s not sick.’ ”
Within a week, he treated another case and saw the same recovery. After five cases, Dr. Sears was confident these were distemper cases being cured. “I kept saying, ‘That’s not possible.’ But I’m looking at it, I’m looking at it, I’m looking at it. These dogs are cured. And so we said, ‘Jesus, we’ve got something really great here.’ ”
In the meantime, Cornell’s report on the serum sample finally came back.
“They wrote back and said ‘It has a very small antiviral activity. We do not suggest using it,’ ” he said. He wrote back to Cornell to report that the serum cleared a dog of distemper within 24 hours. Cornell didn’t respond.
Later, he’d realize one possible explanation for Cornell’s result. The test for interferon is performed in glass tubes – in vitro. He said he suspected that this material works only in vivo – inside a living body, not in a glass tube. Dr. Sears believes the material created by the NDV injection sparks further reactions inside a living dog’s body that work together to neutralize the distemper virus.
A graduate of U.C. Davis veterinary school in 1963, Dr. Sears’ focus was on treating his animal patients and running his business. He had not been instilled with the knowledge of how to seek acceptance, apply for funding for a study and get a new treatment published in a veterinary journal. As a private practice vet working 12-hour days 6 days a week, he was also cut off from the guidance and advice available in academic circles.
So, he drove to a veterinary convention in Las Vegas hoping to share his discovery. However, he came unannounced, without properly documenting his cases or preparing a presentation. During a lecture on canine distemper, Dr. Sears raised his hand, stood up and said, “We have a way to treat distemper.”
He then explained his procedure, the NDV injection, the serum withdrawal, the subcutaneous injection, the dramatic recovery. The expert virologist giving the lecture took this in and paced back and forth on the stage for about a minute and a half.
“Son, that’s impossible. Sit down.”
He fell back into his seat, shattered and dejected. Had someone taken him aside and explained what his presentation lacked and what steps he needed to take next, his story may have turned out differently. Instead, he returned to his clinic and continued to treat dogs but without trying to seek acceptance.
Dr. Sears did find another ally in a related treatment.
The NDV spinal tap
In 1973, Dr. Sears read an article in The California Veterinarian (Adams and Snow 1973) co-authored by John Adams, UCLA’s retired professor of pediatric virology. Adams had been the founding chair of the Department of Pediatrics at the UCLA School of Medicine. A specialist on immunology, multiple sclerosis, and sudden infant death syndrome, Adams had retired in 1972 at the age of 67 but was energetically continuing his research.
The article asked for veterinarians to bring him dogs with Old Dog Encephalitis (ODE) the neurologic stage of canine distemper. Adams had a theory that dogs with ODE were equivalent to people with multiple sclerosis. He believed distemper and measles were equivalent diseases. (Adams et al. 1958) In the 1930s, he’d written one of the first papers on the similarity of distemper and measles. So, Adams saw dogs in the neurologic stage of distemper as an animal model to study measles and MS.
Dr. Sears went to visit Dr. Adams at his UCLA office. “We are in a hotbed of distemper, and I have plenty of cases,” Al said. “Would you be interested?”
“Absolutely, we want as many as we can get,” Adams replied.
While other vets were bringing one or two dogs to Adams, Al brought dozens to UCLA. Adams finally asked, “Why are you getting so many of these cases?” Dr. Sears told him about the widespread cases of distemper in the Antelope Valley but also about the success he had in treating it.
Adams listened. In their long conversations, Adams realized they didn’t just have a chance to understand MS and distemper. If Dr. Al Sears had found a treatment for distemper, then perhaps Dr. Adams might find a treatment for people with MS. But Dr. Sears told him that the NDV serum did not help dogs already in the neurologic stage of the disease.
“So I said it might be worth a try on one of these dogs to put this stuff into the spinal canal to see what we can do,” Dr. Sears said. Adams agreed to perform the first NDV spinal tap, an injection of the Newcastle Disease Vaccine directly into the spinal canal.
On Nov. 14, 1974, Dr. Al Sears brought a 7-year-old Pointer named “Joe” from Rosamond Ca. to Dr. Adams to perform the first NDV spinal tap at the Rigler Research Center in the basement at UCLA.
Dr. Adams wrote in his notes: “When admitted, the dog was unable to walk, pupils were wildly dilated, and the animal appeared to be in acute distress.”
They prepped the dog for surgery and put it under anesthesia. Dr. Sears inserted the needle in the back of foramen magnum, an opening at the base of the skull, which allows access to the spinal canal. From that needle, he withdrew 10 milliliters of cerebrospinal fluid from the spinal canal. Then, 2 milliliters of Newcastle’s Disease Vaccine in solution was injected into the spinal canal.
The injection sent the dog into immediate shock with spasms.
“Well, we all stood there looking at this dog in shock,” Al says. “Since I was clinical veterinarian, I yelled for an IV catheter. I put an IV catheter in him and got this dog on fluids, and of course it recovered in a matter of minutes.”
He left Joe in Dr. Adams care from then on.
In January 1975, Dr. Adams compiled his notes on Joe into a rough draft of a case report.
“In 24 hours, the patient was responding to voice and vocal stimulation,” Dr. Adams wrote. “In 48 hours, the forelegs moved in an attempt to rise, rear legs appeared to be useless and paralyzed.”
In his notes, Dr. Adams reported drawing a new sample of spinal fluid a week after the tap. He sent that off to Cornell for testing. Then, he continued:
“The dog continued to eat and drink well and gradually showed increased muscular activity, forelegs permitted moving to food and water, and the dog made an effort to use his hind limbs, rising partially and collapsing into a lying position. This type of activity has continued, and it is the impression of the examiners that ‘Joe’ is improving very gradually, but still weak and partially paralyzed, particularly in the pelvic limbs. Tail wagging has been noticed by some observers.”
Dr. Adams wrote that as of Dec. 12, nearly a month after the spinal tap, “the patient is continuing to eat and drink lustily and makes a real effort to rise on all fours and to walk, but fails to accomplish this act completely.”
On Dec. 15, he noted, “the dog rose on all fours and ‘walked’ out of his cage for a brief period, but then returned to a prone position. Tail wagging in response to voice.” However, the pupils of his eyes were widely dilated, an indication that he was still having trouble seeing. Then Dr. Adams wrote:
“During the final 2 weeks of December, the dog continued to make slow progress in standing on all four legs and rather vigorous tail wagging when spoken to. He responds to commands and tries very hard to rise on all four legs and manages to walk out of cage area and into the room, which has a tile floor and is slippery, offering very little resistance or help to the animal in his efforts to walk. Vision also appears to be improved, but pupils remain widely dilated except when a bright light is shown into the eye, the pupils responded sluggishly to light.”
On Jan. 2, 1975, Dr. Adams euthanized Joe so that the final spinal, blood and tissue samples could be drawn for the study. The brain, along with a piece of the spinal cord, was removed for Dr. Adams’ research. “Grossly, no distinct lesions could be seen,” he wrote.
Dr. Adams never published the report on Joe’s treatment and recovery. But he continued to explore the possibilities of NDV against distemper, including unpublished experiments using ferrets. “And unfortunately he did something that sort of brought everything to a halt,” Dr. Sears said. “He died.”
Dr. Adams died on June 30, 1980, at age 75. His papers were archived in a box at the UCLA library. Years later, Dr. Sears acquired copies of his notes and papers.
After he died, Dr. Sears contacted the National Institutes of Health and told them about Dr. Adams research. He was told, “Look you’re a veterinarian. We will put you in touch with Cornell, and you can talk to somebody at Cornell.”
When Dr. Sears talked to Cornell Vet School, he said he was told, “Well, send us $500,000, and we’ll initiate a study. We’ll put it in your name.” But as a clinical vet just trying to keep his business afloat, Dr. Sears could not put up such a sum. He said when he called his alma mater, U.C. Davis Veterinary School, and they gave the same answer.
“So, it kind of died,” Dr. Sears said. “And no one else seemed to be interested.”
New supporters of the NDV treatments
Without any allies in the academic world, Dr. Sears focused on running his clinic. For a while during the 1980s, he sold the serum to other veterinary clinics using an Internet billboard service. But as federal regulations on veterinary biologics became more restrictive in the late 1980s, Dr. Sears ended the Internet sales and only used the serum to treat dogs brought to his clinic in Lancaster. After he retired in 2006, he estimated he had treated more than 600 dogs with the distemper and 90 percent of those lived. However, he did not maintain separate records on the treatment of these dogs and he left all his records behind when he retired.
One dog he treated in February 1997 was a Chow-lab mix named Galen, who belonged to Ed and Amy Bond of Los Angeles. Galen was rescued from the streets, and was thought to be about 1 to 2 years old. Within a few days of being rescued, Galen exhibited the respiratory symptoms including coughing, snotty nose, hard pad and a dried up and cracked nasal planum. The Bond’s local vet in Los Angeles diagnosed Galen with distemper but also told them about Dr. Sears’ treatment.
Galen was listless, vomiting and had a fever on the day he was brought to the Sears Veterinary Clinic. He was treated with fluids and antibiotics.
Dr. Sears kept the serum in vials, sealed in plastic bags in a clinic refrigerator. To begin treatment on Galen, he used a syringe to draw 5mls of serum and injected it just under the skin in his rump. Galen got another injection 12 hours later, and a third injection 12 hours after that. The repeated injections are a result of Dr. Sears tinkering with his protocol over the years as he found out what method saved the most dogs. The answer was three shots over 24 hours, each given 12 hours after the previous one. Galen’s fever was under control only 18 hours after the first injection. When he returned to Los Angeles two days later, he was strong and alert. The only visible evidence of the distemper attack was the dry eyes and dry pads of feet, which were treated with ointments over the next few weeks.
At the time, Ed Bond was a reporter for the Los Angeles Times. He attempted to write a feature story about Galen’s recovery but was not able to complete the project before leaving the Times to accept a teaching job. He later posted a draft of the story to the website www.edbond.com in May 2000.
Because of the website, more distemper dogs were brought to Dr. Sears’ clinic for treatment. Thank you notes and owner accounts of recoveries about these treated dogs were posted to the website.[9]
Without Ed Bond’s knowledge, the head of an animal blood bank in Korea read the website in 2003, tested out the NDV serum for himself, found it effective and began offering it as a regular product to his clients in 2004.
In 2011, Dr. Kim Hee Young, senior researcher of the Korean Animal Blood Bank, wrote to Ed Bond:
“… We have used Sears plasma (serum) in Distemper cases
and found it works wonderful. Actually, some of vets had
already used Sears plasma and they recommended to produce this drug. At
the first time, we did not believe that Sears would treat infected or
moderately affected dogs with distemper.
On our first trial (2003), Sears plasma was sent vets to test in Distemper
cases. After sending, we contacted the vets again.
They were good responses about Sears and are still ordering it.
In moderately affected case, we have recommended to use anti-serum
with enough Distemper-antibody together. Their successful rate were more than
60 % (until 2004…. after then, we did not collect data).”
He later followed up with this data:
“In 2003, 102 dogs (from 12 vets) were diagnosed by ELISA[10] as Distemper infection. Of them, the 54 dogs (52 %) were recovered completely on the check-up 6 weeks after Sears treatment. In Korea, the success rate of conventional treatment in case confirmed as Distemper (ELISA) was usually lower than 8 %.”
Beyond the publication of the website and the occasional testimonials from owners, Ed Bond did not initially seek to publish or promote Dr. Sears’ canine distemper treatment. That changed after Dr. Sears retired from his veterinary clinic in 2006 and moved to Utah.
In December 2008, a dog owner in Romania named Mada Lixandru contacted Bond – now living in Upstate New York – to report that her veterinarian had used Dr. Sears’ protocol to make NDV serum and saved at least five dogs with it. Although Bond was not a scientist, this news was significant to him because it meant Dr. Sears’ results could be repeatable.
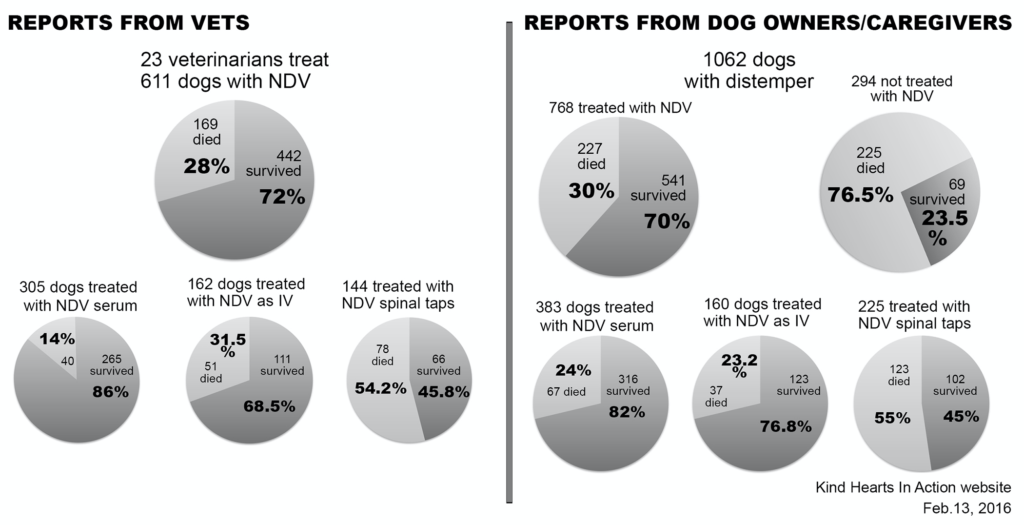
This ultimately led to Bond’s campaign to promote and document Sears’ canine distemper treatments. Using websites and social media, Bond and a newly formed 501c3 charity called Kind Hearts In Action, asked vets, dog owners, rescues and other advocates to consider using Sears’ NDV treatments in distemper cases and report on the outcomes of the cases. Hundreds of cases, including before and after photos and videos, were reported to Kind Hearts In Action between December 2008 and February 2016. This information can only be considered anecdotal because as the information came in from dozens of private practice veterinarians and dog caregivers around the world. Diagnosis and record keeping were not standardized. But the reports were collected in an attempt to demonstrate the potential value of conducting full scientific studies of using NDV against distemper.
Here is a chart on outcomes of treatments, which includes using the NDV serum in pre-neurologic cases, the NDV spinal tap in neurologic cases and another alternate treatment in which the NDV vaccine itself was intravenously injected into the sick dog. This data does not include the report from Korea.
The challenges of proving a treatment to be effective against distemper are daunting. Attempts by private veterinary clinics to properly document their use of these treatments have fallen short because of a lack of time, resources and a need for scientific training that goes beyond standard veterinary experience. The heavy financial costs also are a factor.
“One of the main reasons why fewer drugs exist in veterinary medicine is that FDA’s new drug approval process is very costly and time consuming for pharmaceutical companies, with little return on investment for animal drug products when compared to the return on investment associated with human drug products, creating a relative disincentive for companies to put resources toward creating new veterinary drugs.”[11]
But in one significant example, the NDV spinal tap was performed at Kansas State University’s College of Veterinary Medicine in May 2012. The patient was Nilla, a border collie in the neurologic stage of distemper owned by a pastor and farmer in South Dakota named Clark Audiss.
Audiss’ local vet had scheduled Nilla’s euthanization on Monday, May 7, but instead Audiss took the dog to Kansas State, where Dr. Ken Harkin had approved the procedure, which was performed that Tuesday. Audiss reported that Nilla’s vision began to return during the trip home on Thursday. Over the next few months, Audiss and his family documented Nilla’s recovery on video. By August, Nilla was able to walk, run and herd sheep again. [12]
Audiss brought Nilla back to Kansas State for an evaluation on September 10. Based on that outcome, Dr. Harkin pursued funding for a study of the NDV spinal tap. With support from Maddie’s Fund, Dr. Harkin used the protocol on a handful of dogs between 2014 and 2016, but ultimately concluded the NDV spinal tap was not beneficial.
“No, I do not believe the NDV spinal tap is beneficial and I do believe that the dogs that recovered would have recovered on their own,” Dr. Harkin wrote to Ed Bond.
The key issue was that dogs with myoclonus, the sudden, involuntary jerking of muscles or a group of muscles in many distemper dogs. Nilla did not have myoclonus, but had blindness and paralysis before treatment. Dr. Harkin found that distemper dogs with myoclonus were not helped by the treatment.
“I had a few clients that wanted to come for the study that I convinced to not have the treatment done,” he wrote. “Two of those dogs went on to recover completely with nothing other than good supportive care at home. I know that clients report ‘improvement’ in the symptoms after the treatment, but when they returned here for their recheck I did not appreciate significant improvement in any of them. Maybe there was fractional improvement, but nothing I wouldn’t have expected with time. I do suspect that the NDV vaccine when given intrathecally does cause a transient inflammatory response in the central nervous system (spinal cord, specifically). I think that was manifested in several dogs with significant discomfort/pain that prompted the use of codeine or other analgesic therapy. It is my belief that this inflammation blunts the repetitive firing of the nerves responsible for the chorea (distemper myoclonus). I think that’s why clients see an improvement but I don’t.”
Ed Bond asked, “If Nilla was simply going to have a spontaneous recovery on her own, do you think it possible we are giving up on these dogs too early?”
“I had three dogs that did not have myoclonus: Nilla, Coal, and one other dog. Nilla was the most severely affected,” Harkin replied. “Both dogs recovered completely. Is it possible that the NDV works in a small subset of dogs? I suppose that’s possible, but I doubt it. I think both dogs would have recovered without any therapy. They showed evidence of demyelination and it’s likely that remyelination was happening but that’s a process that just takes time. Early on every dog I saw had a very inflammatory CSF (cerebrospinal fluid), but then post-NDV it would be normal, so I thought the NDV was inducing remission. But, then I had a bunch of dogs that presented with CDV-encephalitis that had completely boring CSF samples, just like the dogs that were post-treatment. It’s just that none of those dogs had been treated. I think the disease can and does go in remission. Interesting, Nilla developed myoclonus long after she left here and recovered. She didn’t have it originally. That myoclonus also eventually subsided. I think we are giving up on some of these dogs way too soon. I have also worked with a shelter in Denver that has saved a number of these dogs with nothing other than good nursing care.”
Future possibilities for treatment and research
In the 20th Century, the approach to a distemper case had been mainly to treat with supportive methods, wait to see if neurologic symptoms began and then euthanize. When an outbreak occurred at a shelter, the response had often been to depopulate – kill every dog in the shelter. Any dog in the neurologic stage of the disease was typically viewed as a lost cause.
Even though the NDV treatments have not been accepted and widely used, there has been a noted shift in the treatment of distemper dogs in the 21st century. Improved methods promoted by Maddie’s Shelter Medicine Program at the University of Florida in distinguishing vaccine titers from hot outbreaks of the disease, isolating and treating sick dogs have given canine advocates hope. At Austin Pets Alive in Texas, many dogs are given the chance to live even when they reach the neurologic stage of the disease.
The data still needs to be standardized but examples from Austin Pets Alive and on the Kind Hearts In Action website show examples of dogs slowly recovering from severe neurologic problems over a matter of months. This may be as a result of the NDV spinal tap, but it may also simply be a matter of neurologic retraining where healthy neurons take over functions from ones damaged by a distemper attack. In these cases, the dogs return to a decent quality of life with chronic but manageable neurologic problems. In any event, the families of these dogs are grateful to still have these pets in their lives. It may be that many of these dogs could be saved if only their vets and owners could give them the time to recover.
In the stats above, dogs in the neurologic stage of distemper treated with the NDV spinal tap showed a survival rate of about 45 percent. Dogs presumably in the pre-neurologic or respiratory stage of distemper who were treated with the NDV serum showed a survival rate of 86 percent, according to the vets.
But this remains anecdotal and to be useful, any scientific study would have to show the treatment dramatically outperforms the known survival rates on distemper from university studies.
In a study at Cornell University in 1984, (Summers et al. 1984) 3- to 4-month old Beagle puppies, bred to be pathogen free, were infected with one of three strains of canine distemper.
• 6 were given Snyder Hill strain
• 11 were given Cornell A75-17 strain
• 12 were given Ohio strain R252
About half of these pups developed neurologic problems and died, but all were eventually euthanized for the study after two months. The Snyder Hill strain, which struck faster, caused a “moribund state” within 14 days and half died from the virus. But some of the Snyder Hill dogs that survived beyond the third week recovered. In the A75-17 group, some dogs reached the moribund stage between the 29th and 38th days. “In both A75-17 and R252 infections, neurologic defects were detectable in about one-half of the dogs.”
In a later collection of papers on paramyxoviruses which cited the Cornell study, “It is claimed that chronic encephalomyelitis with inflammatory demyelinative changes develops in about one-third of dogs experimentally infected with CD virus.” (Randall and Russell 1991) This lines up with Jenner’s original description.
But the disease may be even more deadly outside controlled laboratory studies.
“Distemper is a highly contagious disease that poses a threat mainly to concentrated populations of previously unexposed or unvaccinated, susceptible species. In these populations, distemper is almost always fatal. The disease is complex in that it presents varying clinical symptoms and may run varying clinical courses. Outcomes of CDV infection range from complete recovery to persistent disease to death depending on the age and immune status of the animal infected. Robustness of the humoral immune response correlates with the disease outcome.” (Kapil and Yeary 2011)
An outbreak at a shelter differs quite a bit from a controlled study at a university. The puppies at an infected shelter are being attacked from many directions as their fellow shelter residents shed the virus in multiple ways. In a study, the infection can be given in a controlled way, such as via a single nasal injection and the researchers can take steps to avoid cross-infection from other dogs in the study. Shelter puppies are also likely being attacked by opportunistic infections, such as pneumonia.
In 2020, Cornell’s Wildlife Health Lab website reported that canine distemper “is often fatal with a mortality rate of 50% in adult dogs and 80% in puppies.” [13]
The other problem in proving the value of a canine distemper treatment is that the disease is not reportable so statistics on how many cases occur and how many of those dogs survive are not available. With this major question unanswered, it becomes difficult to build a case for pursuing a study. However, Kind Hearts in Action has received more than 5,000 emails about canine distemper from all over the world in the past 10 years, so cases are still happening and humans are still trying to save their dogs.
The
main question of a study of NDV serum or any potential treatment for canine
distemper should be whether this can prevent distemper dogs from reaching the
neurologic stage of the disease, shorten the course of the disease and
ultimately save more lives than the traditional supportive methods. Any study
would have to show the treatment dramatically outperforms the known survival
rates on distemper from university studies.
BIBLIOGRAPHY
Adams JM, Snow HD. 1973. Viral Demyelinating Encephalitis And Old Dog Encephalitis: Possible Relationship To Distemper Measles, And Dermyelinating Disease Of Man. Calif. Vet. 27: 8-10
Adams JM, Imagawa DT, Chadwick DL, Gates EH, Siem RA. 1958. Relationship of Measles and Distemper. AMA Am J Dis Child.;95(6): 601-608
Ferry N. 1911. Etiology of canine distemper. Journal of Infectious Diseases 4, pp. 399–420.
Jenner E. Observations on the Distemper in Dogs. 1809. Medico-Chirurgical Transactions. 1: 265-270.
Kapil S, Yeary T, 2011. Canine Distemper Spillover in Domestic Dogs from Urban Wildlife. Veterinary Clinics: Small Animal Practice, Volume 4 , Issue 6, pp. 1069-1086.
Kirk H. 1922. Canine Distemper: It’s Complications, Sequelae and Treatment. London. Bailliére, Tindall and Cox.
M’Gowan JP. 1911. Some observations on a laboratory epidemic, principally among dogs and cats, in which the animals affected presented symptoms of the disease called “distemper.” Journal of Pathology and Bacteriology 15, pp. 372 ff.
Oldstone M. 2010. Viruses, Plagues & History: Past, Present and Future. Oxford University Press.
Randall R, Russell W. 1991. Paramyxovirus Persistence Consequences for Host and Virus. In Kingsbury D, editor. The Paramyxoviruses. Springer Science & Business Media. pp. 299-322.
Summers B, Greisen H, Appel M, January 1984. Canine distemper encephalomyelitis: Variation with virus strain. Journal of Comparative Pathology, Volume 94, Issue 1, pp. 65-75
Uhl, E. W., Kelderhouse, C., Buikstra, J., Blick, J. P., Bolon,
B., and Hogan, R. J. (2019). New world origin of canine distemper: interdisciplinary insights.
Int. J.Paleopathol. 24, 266–278. doi: 10.1016/j.ijpp.2018.12.007
[1] Uhl, E. W., Kelderhouse, C., Buikstra, J., Blick, J. P., Bolon, B., and Hogan, R. J. (2019). New world origin of canine distemper: interdisciplinary insights. Int. J.Paleopathol. 24, 266–278. doi: 10.1016/j.ijpp.2018.12.007
[2] Kirk, H. 1922, Canine Distemper: It’s Complications, Sequelae and Treatment. London. Bailliére, Tindall and Cox, pp. 29-34.
[3] Oldstone M. 2010. Viruses, Plagues & History: Past, Present and Future. Oxford University Press. p. 16.
[4] Kirk, p. 66.
[5] Kirk, p. 61.
[6] Kirk, p. 156
[7] Bresalier M, Worboys M. ‘Saving the lives of our dogs’: the development of canine distemper vaccine in interwar Britain. Br J Hist Sci. 2014 Jun; 47(173 Pt 2):305-34. [Online]. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4014013/pdf/S0007087413000344a.pdf
[9] https://edbond.com/distemper_first.html
[10] Enzyme-linked immunosorbent assay
[11] May, K. 2018, Extralabel Drug Use and AMDUCA: FAQ, American Veterinary Medical Association, [Online]. Available: https://www.avma.org/KB/Resources/FAQs/Pages/ELDU-and-AMDUCA-FAQs.aspx
[12] “The Story of Nilla” https://www.kindheartsinaction.com/archives/4130
[13] https://cwhl.vet cited in May 2020.